Cart 0


Long-acting methods: Ethiopia’s next family planning success story
Published on:
Published in:
News
Much has been made of Ethiopia’s dramatic increase in contraceptive use, and rightly so.
In just 15 years, the country went from having one of the lowest modern contraceptive prevalence rates (CPR) in the world at 6.3% in 2000 to 40.4% in 2014, among currently married women.
The country’s progress has largely been driven by innovative community-based programming like the Health Extension Program (HEP). It has been supported by partners like DKT Ethiopia that have complimented public sector distribution. Committed donors that saw an opportunity to invest in high-potential family planning have also been instrumental[1].
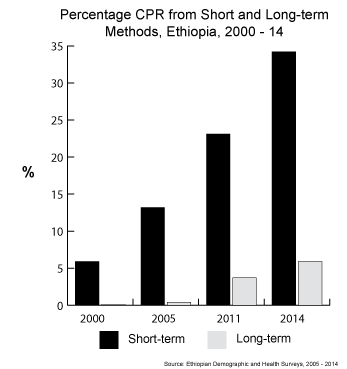
While Ethiopia’s contraceptive growth has thus been rapid and consistently upward, the majority has come from short-term methods like oral pills and injections.
For example, in 2014, injections accounted for 77% of all modern CPR, a rate that has held relatively constant for a decade. Just 15% of CPR came from long-acting reversible contraceptives (LARC) in 2014.
With the Government of Ethiopia now targeting 55% CPR by 2020, of which 35% is expected to come from LARCs, much will need to be done to catalyze uptake of these methods.
Short-term versus Long-acting: What’s the difference?
Short-term contraceptives like pills, injections, and condoms require frequent user action. In the case of pills, users take a tablet daily and must continually obtain new cycles; for injections, users obtain a new injection every three months.
In contrast, LARCs like IUDs and implants can last for years after insertion and require no action on the part of users.
This user independence makes LARCs more effective. Less than 1% of women using implants and IUDs become pregnant per year of use compared to 3% and 8% of women using injectables and pills, respectively[2].
Globally, LARCs account for 27% of all modern CPR and in some countries like China and Egypt, IUDs make up more than half of modern CPR. At the country-level, IUDs, in particular, entail significant cost savings. The average direct cost for a single user of an IUD is $0.58 compared to $4.07 for condoms and $7.51 – 7.90 for hormonal methods[3].
Why are short-term methods so dominant in Ethiopia?
Several factors are likely behind short-term methods making up such a large share of contraceptive use in Ethiopia.
For one, short-term methods do not require the same level of technical capacity to administer as IUDs and implants. In a country that has only recently been able to address the critical shortage of health manpower through the HEP and Human Resources for Health (HRH) Framework, it has not been possible to deliver LARCs at a national scale. With tens of thousands of trained professionals available to provide service, this constraint has largely been dealt with.
LARCs and IUDs, in particular, have also been stymied by misconceptions about the products, both on the part of users and providers. Though decreasingly common, many believe that LARCs cause infertility. A statement by the FMoH’s MCH Directorate indicates that misconceptions like IUDs leaving the uterus and traveling to the brain or causing damage to the male’s anatomy, which are false, persist among some.
DKT and LARCs
As the largest provider of family planning products after the Government of Ethiopia, DKT boasts a full-line of short and long-term contraceptives, the latter including Longact IUDs and Trust implants.
From 2013 to 2015, DKT supplied nearly 900,000 IUDs to the Federal Ministry of Health and non-governmental organizations. This is more than double the 419,350 IUDs imported into the country from 2001 – 2010[4] and foretells of the coming shift to LARCs.
DKT has also begun its own efforts to create demand for LARCs through the private sector. In May 2015, DKT initiated a Partner Clinic pilot with five (5) private maternal and child health (MCH) clinics in Addis Ababa. In eight months, these clinics provided FP to 3,543 women, including delivering 184 IUDs and 207 implants.
According to Solomon Desalegn, MD, GYN/OBS and Owner, Semah OBGYN MCH Center in Addis Ababa, there is a growing demand on the part of consumers for IUDs and implants. “We are seeing more women knowledgeable about IUDs and implants,” says Dr. Solomon.
“As women use the products and talk with each other, we will continue to see interest grow.”
The stage is set
The stage is now set for Ethiopia to make its next mark on global family planning by moving boldly into LARC provision. Already, the national family planning guideline emphasizes activities like “training on next-generation implants” and “ensuring 100% of hospitals and health centers [offer] implants and IUDs by 2020”, which will surely help the country achieve its ambitious LARC target.
ACKNOWLEDGEMENT: A special thanks to Girma Gemechu, Genet Dires, and Tenaya Kebede of the FMoH MCH Directorate for providing background on IUDs in Ethiopia
References
1. Olson D, Piller A. “Ethiopia: An Emerging Family Planning Success Story“, Studies in FamilyPlanning 2013; 44[4]: 445–459
2. Stoddard A. et al. “Efficacy and safety of long-acting reversible contraception,” Drugs, 2011 May 28;71(8):969-80
3. Singh S, Darroch JE and Ashford LS, Adding It Up: The Costs and Benefits of Investing in Sexual and Reproductive Health 2014, New York: Guttmacher Institute, 2014
4. UNFPA. Retrieved from https://www.myaccessrh.org, February 14, 2016.

